PRISMA-symposium, 20 mei 2025
- Rubriek: Congresabstracts
- Identificatie: 2025;10:a1799
Occurrence of potential prescribing cascades after hospital discharge: a cohort study
Johanna H.M. Driessen *, Atiya K. Mohammad, Jacqueline G. Hugtenburg, Alex Marmorale, Carl Siegert, Patricia M.L.A. van den Bemt, Petra Denig and Fatma Karapinar-Çarkit
* Correspondence: annemariek.driessen@mumc.nl.
Background
A prescribing cascade (PC) occurs when a medication (index) causes an adverse drug reaction (ADR), which is addressed by prescribing an additional medication (marker). Medication initiated in the hospital may cause post-discharge ADRs and PCs, especially when multiple healthcare providers are involved.
Objective
The study aimed to assess the cumulative incidence of 20 potential PCs post-discharge and identify the healthcare providers involved in prescribing the marker medication.
Methods
A cohort study was conducted among adult patients admitted to one hospital between 2019 and 2023, who initiated an index medication during their stay. A PC was defined as the initiation of a marker medication which may be intended to treat an ADR induced by the index medication. Data from the hospital and the Nationwide Medication Record System were used to identify potential PCs post-discharge. The primary outcome was the cumulative incidence of PCs, estimated for PCs with ≥ 10 patients initiating the index medication. The secondary outcome was the number of PCs for which ≥ 50% of marker medication was prescribed by a healthcare provider outside the hospital, for PCs with ≥ 10 patients initiating the marker medication. Descriptive statistics were used.
Results
Of 24,282 patients initiating index medication, 502 experienced potential PCs. The cumulative incidence was estimated for 17 PCs, ranging from 0% to 12.3%. For nine PCs, over 50% of marker medications were prescribed by healthcare providers outside the hospital.
Conclusion
The cumulative incidence of potential PCs post-discharge can be substantial with marker medication often prescribed by healthcare providers outside the hospital.
Minderen en stoppen van medicatie bij ouderen middels een medicatiebeoordeling: een cluster-gerandomiseerd onderzoek in de eerste lijn
Gert Baas *, Mette Heringa, Sanne Bakker-Verdoorn, Henk-Frans Kwint, Eman Badawy, Jacobijn Gussekloo, Jako Burgers en Marcel Bouvy
* Correspondentie: g.w.baas@sirstevenshof.nl.
Achtergrond
Polyfarmacie is geassocieerd met een verhoogd risico op bijwerkingen, waaronder (vermijdbare) ziekenhuisopnames. Het minderen of stoppen (deprescribing) van medicatie waarvan de voordelen niet meer opwegen tegen de nadelen, kan bijdragen aan het beperken van bijwerkingen en risico’s, en zo de kwaliteit van leven van de patiënt verbeteren. Een medicatiebeoordeling is een geschikt moment om deprescribing aan te pakken.
Doel
Het onderzoeken van het effect van een medicatiebeoordeling gericht op deprescribing op het aantal in dosering verlaagde en gestopte geneesmiddelen bij ouderen met hyperpolyfarmacie (> 10 chronisch gebruikte middelen) en medicatie op rol.
Methode
Deze cluster-gerandomiseerde gecontroleerde studie werd uitgevoerd in 58 openbare apotheken. Apothekers in de interventiegroep voerden na een medicatiebeoordeling gericht op deprescribing uit bij deelnemende patiënten. De controlegroep leverde standaardzorg. Inclusiecriteria waren patiënten ≥ 75 jaar met hyperpolyfarmacie en medicatie op rol. Op basis van medicatie-aflevergegevens werd het aantal in dosering verlaagde en gestopte geneesmiddelen per patiënt na zes maanden bepaald (primaire uitkomstmaat). Bij start en na zes maanden werden vragenlijsten afgenomen voor secundaire uitkomstmaten, waaronder gezondheidsklachten en kwaliteit van leven (EQ5D-5L/EQ-VAS). Met een generalized linear mixed-model (GLMM) werden de interventie- en controlegroep vergeleken wat betreft de primaire uitkomstmaat en verschillen tussen start en zes maanden.
Resultaten
Tussen oktober 2022 en april 2024 werden 318 patiënten geïncludeerd (55% vrouw, mediane leeftijd 82,4 jaar), verdeeld over de interventieapotheken (n = 155) en de controleapotheken (n = 163). Bij aanvang gebruikten patiënten in de interventiegroep gemiddeld 12,1 medicijnen (standaarddeviatie [SD] = 2,6) en in de controlegroep 11,8 (SD = 2,8). Na zes maanden was het gemiddelde aantal in dosering verlaagde en gestopte medicijnen 2,6 (SD = 1,7) in de interventiegroep versus 1,6 (SD = 1,6) in de controlegroep (P < 0,05). Er was geen verschil in veranderingen in gezondheidsklachten en kwaliteit van leven tussen de groepen.
Conclusie
Een medicatiebeoordeling gericht op deprescribing bij ouderen met hyperpolyfarmacie en medicatie op rol in de eerste lijn leidt tot significant meer in dosering verlaagde en gestopte medicatie in vergelijking met standaardzorg, zonder toename van gezondheidsklachten.
The incidence of diuretic associated sequential prescribing cascades: a feasibility study
K. van der Walle *, K.G.C. Duijts, J.H.M. Driessen, J.T.H. Nielen, F.J.H. Magdelijns, D.L. Weir, P. Denig and F. Karapinar-Çarkit
* Correspondence: kjell.van.der.walle@mumc.nl.
Background
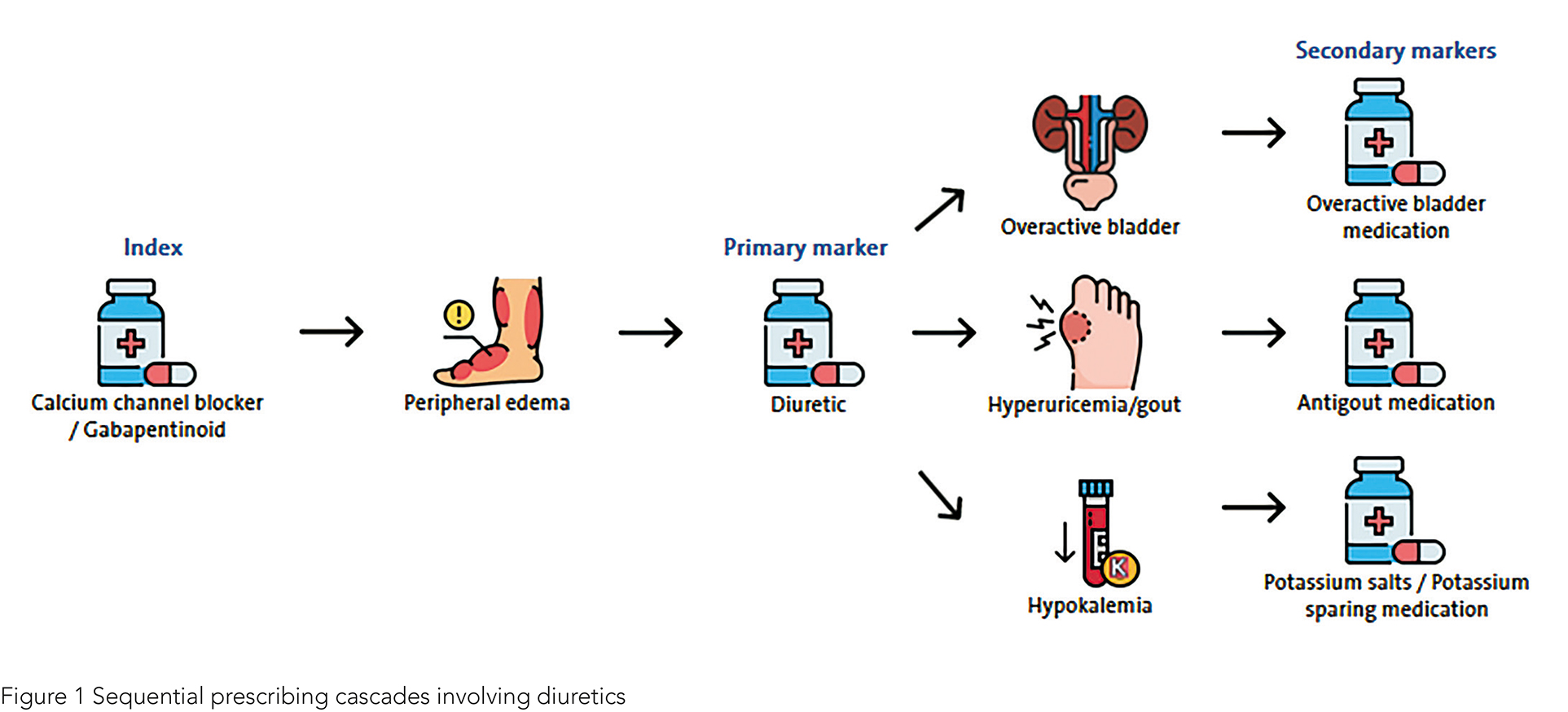
Prescribing cascades occur when adverse drug reactions of a medication (index) are misinterpreted as new medical conditions and subsequently treated with additional medications (marker). They are associated with negative outcomes for patients and health care in general. While individual prescribing cascades involving a single index and marker medication are well-documented, little is known about the occurrence of sequential prescribing cascades (see Figure 1).
Objective
To explore the feasibility of analysing sequential prescribing cascades in large real-world prescription databases by determining their incidence.
Methods
This retrospective cohort study used data from the Clinical Practice Research Datalink (CPRD) to identify patients aged ≥ 65 years who were newly prescribed a diuretic (primary marker) within 12 months of initiating a calcium channel blocker or gabapentinoid (index) between 2018-2022. The incidence of secondary markers prescribed within 12 months after diuretic prescription was determined. Secondary markers included antigout medications, urinary frequency and incontinence medications, and potassium salts and potassium-sparing agents. Selection of index and marker medications was based on the level of evidence of individual prescribing cascades, prevalence of use, registered indications and anticipated prolonged treatment duration of medication.
Results
A total of 608,225 new index users were identified between 2018-2022, of which 28,240 patients (4.6%) were newly prescribed a diuretic within 12 months of their index prescription. Of these, 1,877 (6.6%) were subsequently prescribed one or multiple secondary markers within 12 months of diuretic prescription. Antigout medications were prescribed to 311 patients (1.1%), urinary frequency and incontinence medications to 518 patients (1.8%), and potassium salts or potassium-sparing agents to 1,090 (3.7%) patients.
Conclusion
This study is the first to demonstrate that potential sequential prescribing cascades can be identified in large real-world prescription databases. The substantial amounts of patients experiencing potential sequential prescribing cascades involving diuretics highlight the importance of increased recognition, prevention and management of prescribing cascades in clinical practice.
Dose-dependent relationships observed for prescribing cascades: a cohort study
Sadaf Wahedi *, Ruveyda Gündogan-Yilmaz, Johanna H.M. Driessen, Atiya Mohammad, Petra Denig and Fatma Karapinar-Çarkit
* Correspondence: s.wahedi@olvg.nl.
Background
Prescribing cascades occur when new medications (marker) are prescribed to treat adverse drug reactions (ADRs) caused by an initial medication (index), potentially leading to polypharmacy and increased healthcare costs. The role of the dose of the index medication in the development of these cascades is poorly understood.
Objective
This study investigated the dose-dependent relationship of prescribing cascades for several medications.
Methods
A cohort study using prescription sequence symmetry analysis (PSSA) with data from over 600 pharmacies to examine the relationship between the index medication doses and 18 prescribing cascades, including ACE inhibitors (ACEi), statins, and other medications. Doses were categorized as low (< 0.50 Defined Daily Dose [DDD]), medium (≥ 0.50-≤ 1.50 DDD), or high (> 1.50 DDD). Adjusted sequence ratios (aSRs) > 1 indicated potential prescribing cascades.
Results
Of the 18 prescribing cascades, 12 showed a dose-dependent relationship. All ACEi-related cascades showed strong dose-dependent relationships. For example, ACEi potentially causing cough, showed aSRs increasing from 1.50 (95% confidence interval: 1.32-1.67) to 2.47 (2.37-2.56) from the low-dose to high-dose group, respectively. Other cascades varied in their significance with a dose-response relationship observed for some, such as statins potentially causing erectile dysfunction and urinary tract infections, antidepressants potentially causing urinary incontinence or dihydropyridines potentially causing depression. However, no dose-dependent relationships were identified for proton pump inhibitors, diuretics, or nonsteroidal anti-inflammatory/antirheumatic medications.
Conclusion
High doses of ACEi and statins could potentially contribute to prescribing cascades. Additionally, for some cascades, further research utilizing larger datasets is required to evaluate the dose-dependent relationship. Pharmacists should consider dose reduction to mitigate ADRs and prevent cascades.
Community pharmacist intervention to enhance adherence in patients initiating cardio-vascular medication: the PHARM-ADHERE randomized controlled trial
A. Watteyne *, E. Mehuys, A. Capiau, I. Van Tongelen, P. Pype, E. Van Leeuwen, E. Tommelein, G. Philippe, T. De Backer and K. Boussery
* Correspondence: Adelien.Watteyne@UGent.be.
Background
Poor adherence to cardiovascular (CV) medication is common and significantly contributes to CV morbidity and mortality. The initiation phase is particularly critical, as many patients discontinue key medications within the first year after initiation.
Objective
To investigate whether additional community pharmacist guidance improves adherence in patients starting CV medication.
Methods
A pragmatic 12-week randomized controlled trial was conducted in 204 community pharmacies in Belgium, enrolling adults filling a first prescription for first-line treatments of hypertension, hyperlipidaemia, or type 2 diabetes. Patients were randomized 1:1 to usual pharmacist care or a predefined pharmacist intervention, including protocolled first prescription counselling (patient education and guidance on integrating medication into the daily routine) and a follow-up consultation to proactively tackle adherence issues. Primary outcome was self-reported adherence, using the PROMIS Medication Adherence Scale (PMAS). Secondary outcomes were adherence rate based on dispensing data (using Proportion of Days Covered, PDC) and discontinuation rate.
Results
In total, 883 patients were enrolled with a mean age of 62.6 years and 55.2% were female. Most patients (54.0%) were initiated on an antihypertensive, 36.4% on a lipid-lowering drug and 9.6% on an antidiabetic. About a quarter (25.7%) had a history of a CV event and 20.2% had diabetes. At 12 weeks, self-reported adherence was high in both study groups (median PMAS score: 44), with no significant difference between groups. According to PDC (≥ 80%), 71.2% of patients in the intervention group were adherent compared to 65.5% in the control group. However, this difference was not statistically significant. Treatment discontinuation was significantly lower in the intervention group (17.4%) than in the control group (23.6%; P < 0.05).
Conclusion
Although self-reported adherence and the adherence rate based on dispensing data showed no significant difference between the control and intervention groups, the community pharmacist intervention improved early adherence to CV medication, as indicated by lower discontinuation rates.
Implementatie van het Jaargesprek in dertien apotheken in Vleuten/Leidsche Rijn en Lei-den/Alphen aan den Rijn
Sanne Bakker en Bram Mertens *
* Correspondentie: b.mertens@apotheekstevenshof.nl.
Achtergrond
Steeds meer patiënten met chronische medicatie maken gebruik van de herhaalservice. Dit is een logistiek efficiënt proces in de apotheek met een afhaaltrouw van 100%. Hoe het zit met de therapietrouw is echter onduidelijk. Patiënten geven regelmatig aan dat de aantallen niet kloppen. De vraag of het probleem achter deze niet-kloppende aantallen wordt vaak niet besproken. Bij dit logistieke proces ontbreekt een zorgcomponent.
Doel
Implementatie van het Jaargesprek in dertien openbare apotheken in Vleuten/Leidsche Rijn en Leiden/Alphen aan den Rijn.
Methode
De implementatie is gestart in twee apotheken: Vleuten en Stevenshof. Binnen elke apotheek werd gewerkt met ‘early adopters’: twee apothekersassistenten en één apotheker per locatie startten met de interventie, nadat zij de communicatietraining hadden gevolgd. Nadat het proces goed draaide, werden de volledige teams getraind en betrokken. Na drie tot zes maanden vond een vervolgtraining plaats, waarin ervaringen werden uitgewisseld. Na de pilotfase sloten zeven SARG apotheken in de regio Alphen aan den Rijn en vier FLeiR apotheken aan. Maandelijks werd intervisie gehouden met de projectverantwoordelijke apothekers en de projectleider per regio. Van elk gesprek werden gegevens verzameld via een online formulier.
Resultaten
Gedurende de meetperiode (december 2022 t/m juni 2024) zijn 1905 jaargesprekken geregistreerd. De gemiddelde patiëntleeftijd was 68 jaar en het gemiddeld aantal geneesmiddelen was 5,4. Bij 72% van de jaargesprekken resulteerde het gesprek in een actiepunt. In totaal werden 2290 actiepunten vastgelegd, waarbij er meerdere actiepunten per gesprek mogelijk waren. De meest voorkomende actiepunten waren ‘informatie/advies geven’ en ‘aantallen gelijktrekken’. Daarnaast kwamen ‘voorstel afspraak huisarts’, ‘mogelijke bijwerking’ en ‘innametijden aanpassen’ ook vaak voor. Van de dertien deelnemende apotheken hebben elf apotheken (85%) aangegeven door te gaan met het voeren van de jaargesprekken.
Conclusie
In dertien apotheken is het jaargesprek succesvol geïmplementeerd, waarbij 1905 jaargesprekken zijn gevoerd. De werkwijze met early adopters werkte goed om het proces te optimaliseren en vervolgens uit te rollen. In elf van de dertien apotheken zijn jaargesprekken niet langer een project, maar inmiddels een vast onderdeel van de standaardzorg.
Pharmaceutical discharge letter for patients discharged on combined antithrombotic therapy
Renate van Uden *, Marcia Vervloet, Patricia Pols, Karina Meijer, Patricia van den Bemt and Matthijs Becker
* Correspondence: rvanuden@spaarnegasthuis.nl.
Background
Guidelines recommend using combined antithrombotic therapy for a limited duration. This therapy is most often initiated during hospitalization, with the intended stop date post-discharge. Proper communication of the intended treatment duration to community pharmacies is crucial to avoid unintentional continuation after the stop date.
Objective
To evaluate the impact of a pharmaceutical discharge letter sent to community pharmacies on the unintentional continuation of combined antithrombotic therapy after the intended stop date.
Methods
A pre-post intervention study was conducted at Spaarne Gasthuis hospital, the Netherlands, including patients discharged with combined antithrombotic therapy. In the pre-intervention group (May 2018-August 2019), usual care was provided. In the post-intervention group (August 2020-May 2021), a discharge letter with information about antithrombotic therapy, indication, and stop date was sent to the community pharmacy. The primary outcome was the proportion of antithrombotics dispensed after the intended stop date. Differences between groups were analysed using multivariable logistic regression, adjusted for age, sex, and combined antithrombotic therapy.
Results
In the pre-intervention group, 22.1% (57/258) of all dispensed antithrombotic drugs occurred after the intended stop date versus 9.3% (35/378) in the post-intervention group (adjusted odds ratio [ORadj] 0.31, 95% confidence interval [CI] 0.19-0.51). Among patients with therapy intended for > 1 month, this occurred in 37.8% versus 17.0% (ORadj 0.34, 95% CI 0.20-0.57). In the group of patients with an intended duration > 1 month, for every five letters sent, one unintentional continuation can be prevented.
Conclusion
A pharmaceutical discharge letter reduces unintentional continuation of combined antithrombotic therapy.
De rol van de openbare apotheek in farmaceutische zorg na ontslag: haalbaarheid en effectiviteit van telefonische consulten en huisbezoeken
E.H. Badawy *, M. Heringa, S. Bakker en S. Bakker-Verdoorn
* Correspondentie: e.badawy@sirstevenshof.nl.
Achtergrond
Na ziekenhuisontslag ervaren veel patiënten problemen met medicatiegebruik. Oorzaken zijn beperkingen in de overdracht van medicatiewijzigingen tussen de tweede en eerste lijn en de grote impact van een ziekenhuisopname bij oudere, kwetsbare patiënten met polyfarmacie. Eerder onderzoek heeft aangetoond dat een huisbezoek na ontslag door de eigen openbaar apotheker effectief is bij het opsporen en oplossen van medicatieproblemen, maar ook tijdrovend.
Doel
Het doel van deze studie is het onderzoeken van de effectiviteit van telefonische consulten versus huisbezoeken en bij welke patiënten de interventie het meest zinvol is. Daarnaast wordt de haalbaarheid van brede implementatie in kaart gebracht.
Methode
Het onderzoek werd uitgevoerd in 28 apotheken in Noord-Holland Noord. Patiënten van 65 jaar en ouder die vijf of meer geneesmiddelen gebruikten, kregen binnen een week na ontslag een telefonisch consult (eventueel gevolgd door een huisbezoek) [periode 1] of direct een huisbezoek [periode 2]. Apothekers en farmaceutisch consulenten gebruikten een gestandaardiseerd protocol om medicatiegerelateerde problemen te identificeren en vast te leggen. Tevredenheid van patiënten en zorgverleners werd gemeten via vragenlijsten.
Resultaten
Bij 915 patiënten (44,8% vrouw, gemiddeld 76,3 jaar en 9,5 geneesmiddelen in gebruik) werden consulten na ontslag uitgevoerd: 596 telefonisch (11% gevolgd door een huisbezoek) en 319 huisbezoeken. Huisbezoeken duurden gemiddeld 69 minuten, telefonische consulten 41 minuten. Bij 56% van de telefonische consulten en 80% van de huisbezoeken werd minimaal één medicatieprobleem gevonden (gemiddeld 1,1 versus 1,8 per patiënt; P < 0,001). Meer problemen werden gevonden bij patiënten met medicatiewijzigingen na ontslag en een hoger aantal geneesmiddelen in gebruik. Patiënten en zorgverleners waren positief over de interventie; driekwart van de patiënten gaf aan de medicatie beter te kunnen gebruiken door de interventie.
Conclusie
Bij huisbezoeken na ontslag werden meer medicatieproblemen gevonden dan bij telefonische consulten, maar huisbezoeken kostten ook meer tijd. Problemen kwamen vaker voor bij patiënten met medicatiewijzigingen na ontslag en meer geneesmiddelen in gebruik. Brede implementatie was haalbaar en werd gewaardeerd door zowel patiënten als zorgverleners.
Determinants of appropriate antibiotic use for urinary tract infections in nursing homes – qualitative study of health care professionals’ and residents’ perspectives
Indira Coenen *, Sien Lenie, Kristien Coteur, Carmel Hughes and Veerle Foulon
* Correspondence: indira.coenen@kuleuven.be.
Background
Urinary tract infections (UTIs) are the primary indication for antibiotic use in nursing homes (NHs). Residents are particularly vulnerable to inappropriate prescribing, including excessive prophylactic use, incorrect initiation, and prolonged treatment durations.
Objective
This study aimed to identify key determinants of appropriate antibiotic use for UTIs in NHs by exploring the behaviours and perspectives of all relevant stakeholders.
Methods
We conducted 31 semi-structured interviews with residents/relatives (n = 9), physicians (n = 9), pharmacists (n = 10), and NH management (n = 4), and held 4 focus groups with nurses and nurse aides (n = 25). The Theoretical Domains Framework (TDF) guided the development of the interview guide. Using deductive framework analysis, data were coded to the 14 TDF domains. Inductive content analysis was then applied to identify behavioural determinants within each domain. Key domains for behaviour change were identified based on their importance, relevance, and feasibility, to subsequently inform the design of an intervention.
Results
Appropriate antibiotic use for UTIs in NHs is influenced by a complex interplay of behavioural determinants, with the nursing team playing a central role. Key determinants to address in an intervention include: limited knowledge of guidelines, insufficient self-reflection and monitoring, fear of missing complications, feelings of powerlessness, prioritisation of resident comfort, hierarchical dynamics, social pressure to prescribe, and inadequate support for interprofessional collaboration.
Conclusion
This study identified key behavioural determinants that should be targeted to optimise antibiotic prescribing for UTIs in NHs. These findings underscore the need for a theory-informed, multifaceted intervention to support behaviour change across professional roles and improve antimicrobial stewardship in this setting.
Verantwoording
De hier opgenomen abstracts vormen een selectie uit de presentaties op het PRISMA-symposium van 20 mei 2025 te Amsterdam.
Referentie
Citeer als: PRISMA-symposium, 20 mei 2025. Nederlands Platform voor Farmaceutisch Onderzoek. 2025;10:a1799.
DOI
https://www.knmp.nl/resolveuid/06ef56e5e8164e76ae020ad1fc661fceOpen access

Reactie toevoegen