PRISMA-symposium, 21 mei 2019
- Rubriek: Congresabstracts
- Identificatie: 2020;5:a1722
Availability of information in community pharmacies to warrant correctness of NOAC dosages
S.G.L. Joosten *, C. den Engelsen, H.-J. Guchelaar, and M. Teichert
* Correspondence: sgljoosten@gmail.com.
Background
Guidelines recommend individualized dosing of non-vitamin K oral anticoagulants (NOACs) based on indication and patient characteristics (e.g. renal function).
Objective
To assess whether sufficient information is readily available for community pharmacists to assess correctness of NOAC dosage and whether additional information provided by the general practitioner (GP) is needed in order to do so.
Methods
Cross-sectional pilot study in three community pharmacies and one GP practice without linkage of their computerized systems. Prevalent NOAC users for one GP practice were identified in October 2018 using pharmacy dispensing data. Missing information in the pharmacy system was collected from GP patient files. Data were analysed by descriptive statistics in Excel.
Results
Of 108 prevalent NOAC users (mean age = 74 [range = 19-96], 55% women), the pharmacy system yielded information on recent renal function measures in 26 (24%) patients. For none of the patients information on indication or body weight was available. Additional information from the GP system enabled dosage assessment in 96 (89%) patients. For 12 (11%) patients information on recent patient measures (9), indication (1) or both (2) was lacking in both the pharmacy and GP systems. Of 96 patients with sufficient information, 79 (82%) received guideline adherent dosages, 11 (11%) too high and 6 (6%) too low dosages.
Conclusion
Information on parameters needed for individualized dosing of NOACs is insufficiently available for community pharmacists. This study highlights the need to share information on indication and patient measures and its potential in contributing to safe and effective use of NOACs.
Voorschrijven van dubbele antistollingstherapie volgens de richtlijnen; een interventie studie
R.C.A.E. van Uden *, H.J. Kingma, D.A.M. Odekerken, P.M.L.A. van den Bemt en M.L. Becker
* Correspondentie: ruden@sahz.nl.
Achtergrond
Gebruik van antistolling is een fragiel evenwicht tussen het risico op bloedingen en trombotische events. Dubbele en triple antistolling geeft een twee tot vier keer hoger bloedingsrisico dan monotherapie. Daarom adviseren richtlijnen om dubbele en triple antistolling voor een beperkte periode te gebruiken.
Doel
Bepalen hoeveel patiënten conform de richtlijnen worden behandeld met dubbele of triple antistolling.
Methoden
Een prospectieve interventiestudie werd uitgevoerd tussen mei 2018 en februari 2019. Een apotheker evalueerde dagelijks alle patiënten ouder dan 18 jaar die dubbele of triple antistolling gebruikten. Indien zij niet volgens de richtlijnen werden behandeld, werd overlegd met de voorschrijver over het antistollingsbeleid.
Resultaten
446 patiënten werden geïncludeerd, waarvan 209 (46,9%) patiënten werden behandeld volgens de richtlijnen en bij 237 patiënten (53,1%) werd hiervan afgeweken. Van de afwijkende patiënten werd bij 16 patiënten bewust afgeweken (6,8%), bij 13 patiënten (5,5%) is geen contact geweest met de voorschrijver. Bij de overige 208 patiënten (46,6%) zijn 229 adviezen over het antistollingsbeleid gegeven, waarvan 226 adviezen (98,7%) zijn opgevolgd. Na interventie werden significant meer patiënten volgens de richtlijnen behandeld dan ervoor (P < 0,0001). Een direct oraal anticoagulans en een laagmoleculair gewichtsheparine werd bij 135 patiënten (64,9%) gelijktijdig voorgeschreven. 66 patiënten (31,7%) hadden geen indicatie voor een trombocytenaggregatieremmer naast een oraal anticoagulans.
Conclusie
Bij 46,6% van de patiënten die dubbele en triple antistolling gebruiken wordt onbewust afgeweken van de richtlijnen. Evaluatie van het antistollingsbeleid door een apotheker heeft meerwaarde bij deze patiënten.
Use of direct oral anticoagulants in a real-world setting: a community pharmacy-based study
A. Capiau *, E. Mehuys, I. Van Tongelen, T. De Backer, T. Christiaens, A. De Sutter, S. Steurbaut, S. Moudallel, S. Rydant, and K. Boussery
* Correspondence: Andreas.Capiau@UGent.be.
Background and objective
Despite the numerous RCTs with direct oral anticoagulants (DOAC), further follow up on how this high risk new drug class is used in real-world clinical practice is warranted. This study aimed to describe DOAC use in a primary care sample of long-term users and investigated: adherence, patients’ perceptions, drug interactions, and appropriateness of dosing.
Methods
A cross-sectional observational study was conducted in 158 community pharmacies. Participants were home-dwelling adults treated with DOAC for at least one year. Adherence to DOAC (self-reported (Medication Adherence Report Scale, MARS) and calculated using pharmacy dispensing data (Medication Possession Ratio, MPR); patients’ perceptions about DOAC (Beliefs about Medicines Questionnaire, BMQ); and prevalence of drug interactions and inappropriate dosing (using the recommendations in the summary of product characteristics (SmPC) and the 2018 European Heart Rhythm Association (EHRA) Practical Guide) were assessed.
Results
Of the 766 participants 40.5% used rivaroxaban, 36.2% apixaban, 21.1% dabigatran and 2.2% edoxaban. Adherence to DOAC was high (mean MARS score = 24.6 ± 1 and 85.4% of patients with MPR ≥ 80%). BMQ showed that 91.3% of patients favoured the ‘necessity’ over the ‘concerns’. Thirty- one percent of patients had ≥ 1 drug interaction(s) with DOAC. DOAC dosing was inappropriate in 15.4% of patients according to SmPC and in 23.1% according to EHRA.
Conclusion
This real-world analysis of DOAC use revealed high adherence and necessity beliefs, drug interactions in 30% of patients, and suboptimal dosing in about one fifth of patients. These findings can inform the design of targeted community pharmacist interventions to improve quality of DOAC use.
Post-discharge medication-related problems in a cardiac population: a pharmacist-community care registered nurse collaboration
S. Daliri *, A. El Mokaddam, B.M. Buurman, P. Jepma, L. Verweij, W.J.M. Scholte op Reimer, and F. Karapinar-Çarkit.
* Correspondence: s.daliri@olvg.nl.
Background
The risk of medication-related problems (MRPs) is increased in cardiac patients post-discharge. Community care registered nurses (CCRNs) can detect issues that indicate the occurrence of MRPs. The knowledge of pharmacists on medication can add to the quality of medication-related care.
Objective
To study the effect of a pharmacist and CCRN collaboration during post- discharge home visits on the type and occurrence of post-discharge MRPs in a cardiac population.
Methods
An observational prospective study was conducted as part of an ongoing randomized controlled trial ‘Cardiac Care Bridge’ in 5 Dutch hospitals. Intervention group patients, who received pre- and post-discharge care, were included. Post- discharge, they received 4 home visits by CCRNs who reconciled medication and observed signs and symptoms with a validated ‘alarm symptom’ list. A pharmacist supported the CCRNs and reported additional signals, recommended interventions, and assessed the occurrence of potential MRPs. All data were analysed using descriptive statistics.
Results
In total, 78 patients were randomized to the intervention group. Complete data were available in 56 patients (72%). During the first home visits, a total of 431 signals were reported: 238 (55.2%) from the alarm list (mainly cardiac symptoms), 103 (23.9%) from the pharmacist (e.g. use of medication with no apparent indication), and 90 (20.9%) from medication reconciliation (e.g. discrepancies in medication use at home compared to the discharge letter). In total, 171 signals (39.7%) were classified as MRPs.
Conclusion
This research shows that MRPs post-discharge occur frequently in the cardiac population. The collaboration between the pharmacist and CCRN allows for early detection of potential MRPs.
Klinische relevantie van door apothekers uitgevoerde farmacotherapeutische receptwijzigingen
Ellen van Loon *, Mette Heringa, Annemieke Floor-Schreudering, Marcel L. Bouvy, Henk Buurma, Toine C.G. Egberts en Peter A.G.M. de Smet
* Correspondentie: wevanloon@kadds.nl.
Achtergrond
Landelijk onderzoek uit 2016 liet zien dat openbaar apothekers gemiddeld 6,5 farmacotherapeutische receptwijzigingen per dag doorvoeren. De relevantie van deze wijzigingen geeft een indicatie van de bijdrage van de openbaar apotheker aan de kwaliteit van de farmacotherapie.
Doel
Het vaststellen van de klinische relevantie van door openbaar apothekers doorgevoerde farmacotherapeutische receptwijzigingen.
Methoden
Een panel van vijf openbaar apothekers, vijf ziekenhuisapothekers, vijf huisartsen, vijf internisten/geriaters en vijf niet-praktiserend deskundigen schatte de relevantie in van 160 praktijkcasus betreffende farmacotherapeutische receptwijzigingen. De 25 panelleden beoordeelden ieder 32 casus in een online vragenlijst. Elke casus werd door één panellid van elke discipline beoordeeld. Per casus werd de algemene relevantie en het effect op de gebieden effectiviteit, veiligheid, doelmatigheid en gebruiksgemak uitgevraagd.
Resultaten
Er werden 16 casus geëxcludeerd waarbij drie of meer beoordelaars de beschikbare casusinformatie onvoldoende vonden voor de relevantiebepaling. Bij 56,3% van de casus werd de farmacotherapiewijziging beoordeeld als relevant en bij 4,2% als uiterst relevant. De overige casus werden als matig relevant (31,9%) beoordeeld, of de beoordeling was niet eenduidig (7,6%). Bij
25% van de casus was er sprake van een grote verbetering op minimaal 1 van de aspecten veiligheid, effectiviteit, gebruiksgemak of doelmatigheid. De verbeteringen waren ongeveer gelijk verdeeld over deze aspecten.
Conclusie
Ruim 60% van door de openbaar apotheker doorgevoerde farmacotherapeutische receptwijzigingen werd als klinisch relevant tot uiterst relevant beoordeeld. Dit komt overeen met 3,9 klinisch (uiterst) relevante farmacotherapiewijzigingen per apotheek per dag.
Onbetrouwbare bloedglucosemeters en gebruiksfouten bij bloedglucosemetingen
E.C. Weening *, J.S. Klever, P.M. Malingré en C.C.M. Schuiling-Veninga
* Correspondentie: e.c.weening@rug.nl.
Achtergrond
In Nederland zijn circa 260.000 diabetespatiënten dagelijks afhankelijk van insuline. Deze patiënten prikken regelmatig hun bloedglucosewaarde met een bloedglucosemeter. Uit verschillende onderzoeken blijkt dat deze meters vaak een (te) grote afwijking vertonen en daarmee niet de juiste waarde geven. Ook het niet correct uitvoeren van een meting is van grote invloed op de gemeten waarde.
Doel
Bepaling van de nauwkeurigheid van bloedglucosemeters en bepaling van het aantal en type fouten in bloedglucosemetingen door patiënten.
Ontwerp en methoden
398 patiënten die dagelijks insuline gebruiken zijn uitgenodigd voor een controle van hun bloedglucosemeter. De controle bestond uit 2 onderdelen. Allereerst heeft de patiënt zelf een bloedglucosemeting uitgevoerd met gebruikmaking van de eigen bloedglucosemeter. Tijdens de uitvoering zijn vier aspecten gecontroleerd: handen wassen, gebruik nieuwe lancet, direct sluiten van container met teststrips, en niet op vinger drukken. Vervolgens is een referentiemeting uitgevoerd met de volgende druppel bloed met de StatStrip Xpress-referentiemeter. Volgens ISO 15197: 2013-norm moest het verschil tussen beide metingen minder zijn dan 15%.
Resultaten
In totaal hebben 113 patiënten deelgenomen en zijn 113 bloedglucosemeters van zes verschillende merken gecontroleerd. De bloedglucosemeting van 9 patiënten week meer dan 15% af van de referentiemeting. 52,2% van de patiënten maakte ten minste één fout tijdens de uitvoering van de bloedglucosemeting. De meest voorkomend hierbij: het niet wassen van de handen (33,6%) en het indrukken van de vinger (27,4%).
Conclusie
Ongeveer 8% van de bloedglucosemetingen levert een onbetrouwbare bloedglucosewaarden op conform de ISO-norm.
Medication related readmissions within 30 days after discharge: preventability, causes and risk factors
E.B. Uitvlugt *, Dr. M.J.A. Janssen, Dr. C.E.H. Siegert, Dr. E.L. Kneepkens, Dr. B.J.F. van den Bemt, Prof. dr. P.M.L.A. van den Bemt, and Dr. F. Karapinar-Çarkit
* Correspondence: e.uitvlugt@olvg.nl.
Background
Little is known about the proportion of all readmissions that are medication related and the preventability of these medication related hospital readmissions
Objective
Primary aim: to assess the percentage and preventability of readmissions within 30 days of discharge caused by medication. Secondary aims: to assess causes of preventable medication related readmissions and associated risk factors.
Methods
Patients with a 30-day unplanned hospital readmission from seven participating departments of a Dutch teaching hospital were included. Residents and a pharmacist reviewed medical records of patients and assessed whether the readmission was medication related and preventable. During multidisciplinary meetings preventable cases were discussed and consensus was reached. Causes were assessed for preventable readmissions. To assess potential risk descriptive statistics were used. †
Results
874 readmissions were included. Nineteen percent (n = 166) was medication related and of these, 35% (n = 58) was potentially preventable. Causes of these readmissions were problems due to prescribing (47%), patient non-adherence (29%) and transfer of medication related information (24%). Patients with a potentially preventable readmission had a significantly higher age (70 versus 63 years), used more medicines (11 versus 8.8), had a longer length of index admission (7.5 versus 4 days) and more often had a renal clearance < 50 mL/min (31% versus 18%) compared to patients with a readmission not caused by medication.
Conclusion
Nineteen percent of readmissions is caused by medication, and of these 35% were potentially preventable. Causes and associated factors identified in this study could be helpful to implement interventions to reduce readmissions.
† Logistic regression analysis is in progress.
The effect and clinical impact of a longitudinal medication reconciliation service: a prospective multicentre observational study
S. Daliri *, M. Bouhnouf, H.W.P.C. van de Meerendonk, B.M. Buurman, W.J.M. Scholte op Reimer, M.J. Kooij, and F. Karapinar-Çarkit
* Correspondence: s.daliri@olvg.nl.
Background
Medication reconciliation (MR) is a widely recognized method to promote patient safety at care transitions. Currently, studies focus on reconciling differences between medication lists instead of creating adequate lists. Furthermore, MR is not performed longitudinally in the healthcare continuum.
Objective
To assess the proportions of patients for whom at least one intervention is initiated during MR at hospital admission, hospital discharge and in the home setting, and to assess the clinical impact of these interventions.
Methods
A prospective observational study was conducted in two Dutch hospitals. Patients discharged from the internal medicine, cardiology, neurology and pulmonology departments were included, and received MR at admission, discharge and within 5 days after discharge at home. MR interventions were classified as discrepancies (unintentional differences between actual and documented medication use), optimizations (adhering to guidelines), and patient-handling interventions (improvement of medication use by patients). Using a validated instrument, the clinical impact of MR interventions was determined independently by an expert panel. Data were analysed using descriptive statistics.
Results
In total, 197 patients were included (median age = 73 years). At hospital admission, in 66.5% of patients interventions were initiated, mostly due to identified discrepancies. At hospital discharge, in 80.7% of patients, mostly to optimize pharmacotherapy. In the home setting, mostly patient-handling interventions were initiated (97.5%). In 161 patients (81.7%) at least one intervention was implemented to overcome significant, serious or potentially lethal medication errors.
Conclusion
Longitudinal MR is needed as different interventions are initiated at transitions in care. At discharge, medication errors have the highest potential to jeopardize patient safety.
Patient involvement in medication management in nursing homes
Amber Damiaens *, Annelies Heylen, Marijke Vanbillemont, and Veerle Foulon
* Correspondence: amber.damiaens@kuleuven.be.
Background
Research has shown that interdisciplinary case conferences (ICC) are an effective strategy to optimize the medication use of nursing home residents (NHRs). This has recently been confirmed in the COME-ON study, a RCT in Belgian nursing homes that investigated the impact of a medication review performed by the GP, pharmacist and nurse. Although the intervention was patient-centered in its aim, it was not patient-centered in its approach, since neither NHRs nor informal caregivers were present during the case conferences.
Objective
To investigate the experiences and expected level of involvement of NHRs and their caregivers in medication management.
Methods
Focus groups with NHRs and caregivers were organized.
Results
Four focus groups with residents and four with caregivers were performed. Trust in the GP was a key element for NHRs, resulting in a kind of resignation. However, NHRs expected clear communication about medication changes. Residents expressed concerns for participation in ICC, with regard to the language that would be used and the time management of the GP. For the informal caregivers it seemed important that information about medication is shared spontaneously. They strongly felt the need to be more informed about (changes in) medication of the resident they care for, and showed some willingness to participate in ICC.
Conclusion
Caregivers are more in favor of participating in ICC concerning the medication of the resident, than NHRs themselves. Residents have concerns about playing an active role, but want to be thoroughly informed about (changes in) their medication.
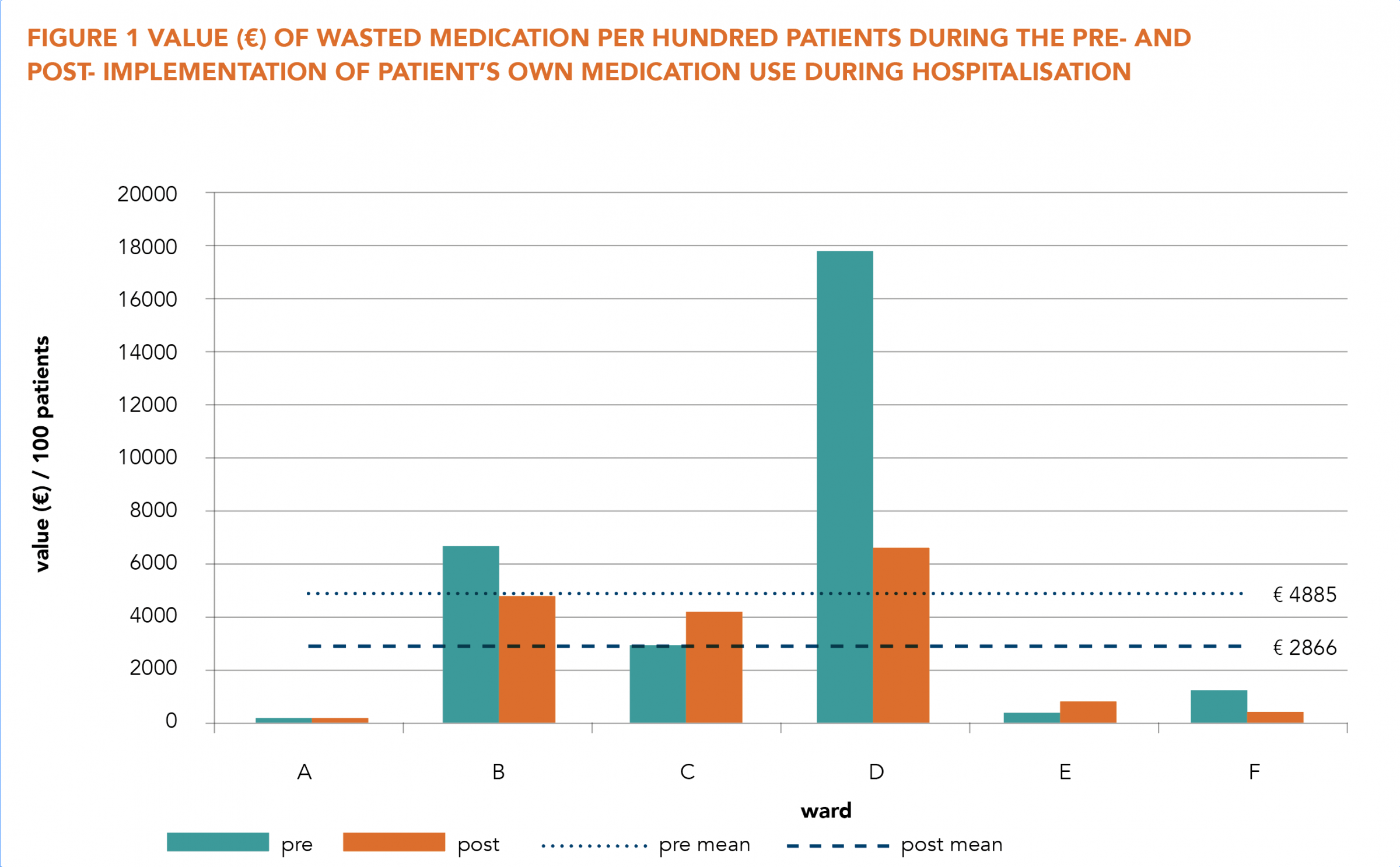
Economic impact of implementing patient’s own medication use during hospitalisation: a multicentre pre-post implementation study in Dutch healthcare
L.J.M. van Herpen-Meeuwissen *, B.J.F. van den Bemt, B. Maat, and H.A.W. van Onzenoort
* Correspondence: Loes.vanHerpen-Meeuwissen@radboudumc.nl.
Background
Medication is frequently being wasted, for example after patient’s discharge from hospital. This wastage has undesirable economic and environmental consequences. Continuation of Patient’s Own Medication (POM) during hospitalisation may reduce medication waste and also decrease time spend by hospital staff on the medication process (MP).
Objective
To investigate the economic impact of POM during hospitalisation on medication waste and hospital staff’s time spend.
Methods
This prospective pre-post intervention study was conducted at seven wards, including surgical and medical wards. Data were collected for two months at a time. Medication waste, defined as value (€) of wasted medication per hundred patients, was measured by identifying all disposed medication. Time spend on MP tasks by hospital staff was measured ten times per ward per staff member. Total mean time spend on the MP (per staff member) per hundred patients was calculated for the pre- and post-implementation MP.
Results
The mean value of wasted medication was € 4885 versus € 2866 per hundred patients, during pre- and post-implementation of POM respectively (figure 1); a decrease of 41.3%. The mean time spend on the MP increased, namely 8197 versus 8275 minutes per hundred patients. A change in division of tasks was observed, as physicians and nurses spend less time and pharmacy practitioners had a greater role in the MP. When time effort was correlated to salary € 1731 could be saved per hundred patients.
Conclusion
This study shows that POM implementation may have a positive economic impact, as the value of medication wasted decreases and staff deployment is more efficient.
Kosteneffectiviteitsanalyse van een medicatiebeoordeling gericht op persoonlijke wensen en doelen van de patiënt: economische evaluatie van de DREAMeR-studie †
Sanne Bakker-Verdoorn *, Jeroen van de Pol, Anke Hövels, Henk-Frans Kwint, Jeanet Blom, Jacobijn Gussekloo en Marcel Bouvy
* Correspondentie: s.verdoorn@apotheekhoogland.nl.
Achtergrond
Het aantal ouderen met polyfarmacie neemt toe, wat kan leiden tot hoge zorguitgaven in de toekomst. Mogelijk kan een medicatiebeoordeling zorgkosten besparen, maar het is ook een tijdsintensieve interventie die mogelijk juist kosten zal verhogen.
Doel
Het doel van dit onderzoek was om de kosten effectiviteit te bepalen van een medicatiebeoordeling.
Methoden
Een kosteneffectiviteitsanalyse werd uitgevoerd vanuit een maatschappelijk perspectief, als onderdeel van de DREAMeR studie: een gerandomiseerd gecontroleerd onderzoek uitgevoerd bij ouderen van ≥ 70 jaar die ≥ 7 geneesmiddelen gebruikten. De interventiegroep ontving een medicatiebeoordeling gericht op persoonlijke wensen en doelen van de patiënt en de controlegroep ontving standaardzorg. Zorgconsumptie en geneesmiddelgebruik werden verzameld over een periode van zes maanden om de zorgkosten te berekenen. Effecten werden gemeten als quality adjusted life years (QALY’s) met EQ-5D en EQ-VAS en als aantal afgenomen gezondheidsklachten per patiënt na zes maanden.
Resultaten
De totale gemiddelde zorgkosten per patiënt over zes maanden waren € 4189 ± 6596 in de controlegroep (n = 294) en € 4008 ± 6678 in de interventiegroep (n = 294), inclusief interventiekosten die werden vastgesteld op gemiddeld € 199 ± 67 per patiënt. Dit resulteerde in een incrementele kosten besparing van € 181 in de interventiegroep t.o.v. de controlegroep. De gemiddelde incrementele QALY’s na zes maanden waren: 0,00217 voor EQ-5D, 0,00363 voor EQ-VAS en 0,33 gezondheidsklachten voor de interventiegroep ten opzichte van de controlegroep. De probabilistische sensitiviteitsanalyse liet zien dat er een kans van > 90% was dat een medicatiebeoordeling kostenbesparend is. Een medicatiebeoordeling was de dominante strategie voor de kosten/QALY gemeten met EQ-VAS en de kosten/gereduceerde gezondheidsklacht.
Conclusie
Een medicatiebeoordeling is een economische aantrekkelijke interventie bij deze doelgroep vanwege de grote kans op kostenbesparing in combinatie met positieve effecten op kwaliteit van leven (EQ-VAS) en gezondheidsklachten.
† DREAMeR: Drug use Reconsidered in the Elderly using goal Attainment scales during Medication Review.
Investigating education and counselling for patients treated with oral anticancer drugs: patients’ perceived satisfaction with information about medicines
Lise-Marie Kinnaer *, Ann Van Hecke, and Veerle Foulon
* Correspondence: lisemarie.kinnaer@kuleuven.be.
Background
Treating cancer patients with oral anticancer drugs (OACD) causes a shift in responsibilities from the oncology team to the patient. Therefore, patient counselling should focus on adequate self-management.
Objective
To investigate the level of patient satisfaction with provided information about OACD during counselling with health care professionals (HCPs) in the hospital.
Methods
A multicenter cross-sectional study using Satisfaction with Information about Medicines Scale (SIMS) was set up. All patients, aged 18 years or older, who started an oral anticancer treatment for the first time, were requested to complete the SIMS three days after the start of the therapy. SPSS was used to analyse the data.
Results
In total, 60 patients completed the questionnaire. The overall scores on the SIMS showed that 50.8% of patients were dissatisfied about the provided information, mostly on the following elements: how long it will take before the drug works, duration of the treatment, risk for side effects, interference with sex life and alcohol, drowsiness, interference with other medicines and what to do in case of a missed dose (7 out of 16 items).
Conclusion
A considerable number of patients reported that the information on OACD was not sufficient. Healthcare professionals (HCP) might not be aware of all relevant aspects of oral anticancer therapies that need to be discussed. To overcome this barrier, dedicated patient leaflets that structure the consultation as well as training in counseling competencies might be helpful. This is currently tested in a before-after study in four hospitals.
Effectiviteit van de MyPuff-app bij patiënten met astma en/of COPD in het verbeteren van de inhalatietechniek
Anna Vanoverschelde *, Paulien van der Wel en Lies Lahousse
* Correspondentie: Anna.Vanoverschelde@UGent.be.
Achtergrond
Patiënten met astma en/of COPD hanteren frequent een incorrecte inhalatietechniek met een verminderde ziektecontrole tot gevolg [1]. Hoewel reeds werd aangetoond dat farmaceutische zorgprogramma’s in België de inhalatietechniek bij COPD patiënten kunnen verbeteren [2], werd de integratie van de MyPuff-app om de inhalatietechniek thuis verder te oefenen nog niet geëvalueerd.
Doel
De effectiviteit van de MyPuff-app onderzoeken in het verbeteren van de inhalatietechniek bij astma en/of COPD patiënten.
Methoden
Een drie maanden durend gerandomiseerd gecontroleerd onderzoek werd uitgevoerd in 9 officina-apotheken in België. Patiënten met astma en/of COPD werden van maart tot oktober 2018 gerekruteerd. Patiëntkarakteristieken, exacerbatiehistorie en ziektecontrole werden bevraagd. De gedemonstreerde inhalatietechniek werd beoordeeld via vergelijking met het juiste protocol per inhalator. Fouten werden als kritisch beschouwd indien ze de longdepositie substantieel wijzigen [3].
Resultaten
Zeventig patiënten (mediane leeftijd = 64 jaar, 56% ♀, 31 met astma [44%], 27 met COPD [39%], 12 met ACO [17%]) werden gerandomiseerd tot de app (n = 37, 53%) of de informatiefolder (n = 33, 47%). Bij de 60 patiënten met follow-up verbeterde de gemiddelde score op inhalatietechniek statistisch significant (+16%). De verbetering van de inhalatietechniek was niet hoger in de interventiegroep (gebruik = 13%) dan in de controlegroep (gebruik = 57%). Gecorrigeerd voor leeftijd, geslacht, BMI en rokersstatus, waren kritische fouten in de inhalatietechniek geassocieerd met exacerbaties (OR = 3,5, 95%-BI = 1,1-11,5, P = 0,039).
Conclusie
De inhalatietechniek van astma en/of COPD patiënten was significant verbeterd drie maanden na de geleverde farmaceutische zorg. Echter, de meerwaarde van de MyPuff-app tegenover een informatiefolder om de inhalatietechniek thuis verder te oefenen, kon niet aangetoond worden in deze studie.
Verantwoording
De hier opgenomen abstracts vormen een selectie uit de presentaties op het PRISMA-symposium van 21 mei 2019 te Amersfoort.
Literatuur
1. Sanchis J, et al. Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150(2):394-406.
2. Tommelein E, et al. Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): a randomized controlled trial. British journal of clinical pharmacology. 2014;77(5):756-66.
3. Usmani OS, et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes. Respiratory research. 2018;19(1):10.
Referentie
Citeer als: PRISMA-symposium, 21 mei 2019. Nederlands Platform voor Farmaceutisch Onderzoek. 2020;5:a1722.
DOI
https://www.knmp.nl/resolveuid/52f98a04f13144d58c05c9aaed4b41afOpen access

Reactie toevoegen